Glenohumeral instability may arise from an acute injury or develop into a chronic condition due to repeated trauma. The most common form is anterior instability, typically following a glenohumeral dislocation or subluxation. Posterior instability is less common but occurs more frequently in contact athletes, such as those who play football or lacrosse. Superior labral tears (SLAP lesions) do not usually result in instability but can significantly impact overhead athletes and manual laborers due to pain and functional limitations.
Multidirectional instability (MDI) is generally considered a congenital condition, often associated with underlying systemic disorders such as collagen/soft-tissue laxity disorders. In MDI, global capsular laxity and labral insufficiency are seen.
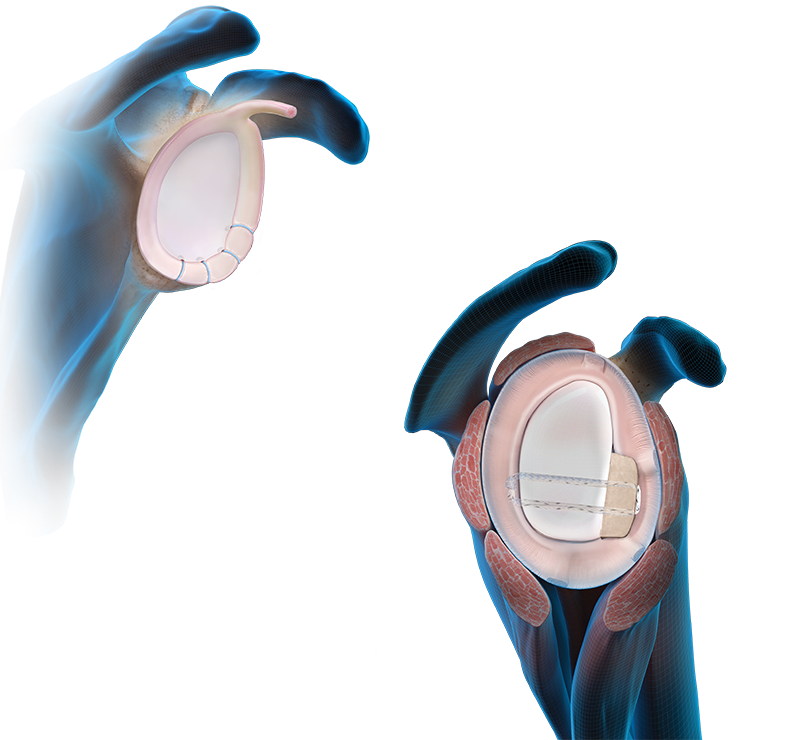
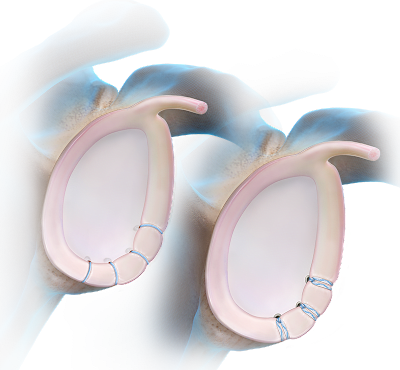
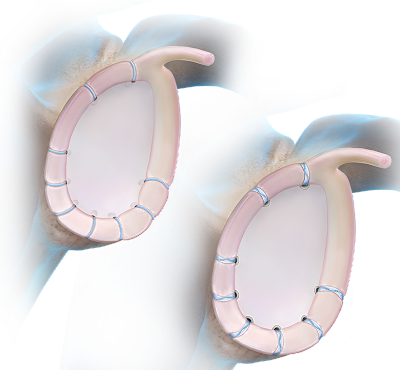
Glenohumeral instability occurs when the glenoid labrum and surrounding ligaments are stretched or torn. This often results in a Bankart lesion, which may occur with or without associated glenoid bone loss. Additional lesions contributing to anterior instability include humeral avulsion of the glenohumeral ligament (HAGL) and anterior labroligamentous periosteal sleeve avulsion (ALPSA).
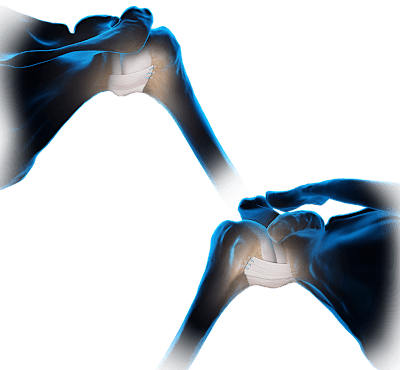
Posterior instability is commonly associated with reverse Bankart lesions, which involve detachment of the posterior labrum.
Arthrex has developed specific techniques to address each type of instability.
Please note that certain bio (PLLA) anchors and screws are not available for sale in EMEA.